











TL;DR:
- Mushroom allergenicity involves IgE-mediated responses to proteins in fungi, causing rapid skin, respiratory, and digestive symptoms. Accurate diagnosis requires component-resolved testing and clinical history to distinguish true allergies from dermatitis or sensitivities. Management includes personalized allergist evaluation, careful label reading, and thorough cooking to prevent adverse reactions.
Mushroom allergenicity is defined as an IgE-mediated immune response to specific proteins found in edible fungi, triggering allergic reactions that can affect the skin, respiratory tract, and digestive system within minutes to hours of exposure. Species like shiitake (Lentinula edodes) and maitake (Grifola frondosa) are among the most commonly implicated in reported reactions, though any edible mushroom can provoke sensitization in susceptible individuals. Symptoms range from mild hives and nasal congestion to severe anaphylaxis. The American Academy of Allergy, Asthma, and Immunology recognizes fungi as a clinically significant allergen category, and understanding the difference between a true IgE-mediated allergy and other mushroom reactions is the first step toward safe, informed choices.
What causes mushroom allergenicity and how does the immune system react?
Mushroom allergenicity begins when the immune system misidentifies proteins in mushroom tissue or spores as harmful. On first exposure, the body produces IgE antibodies specific to those proteins. These antibodies attach to mast cells throughout the body. When mushroom proteins are encountered again, they bind to those IgE antibodies and trigger mast cells to release histamine and other inflammatory chemicals. This cascade is what produces allergic symptoms including hives, wheezing, nausea, vomiting, and in severe cases, anaphylaxis.
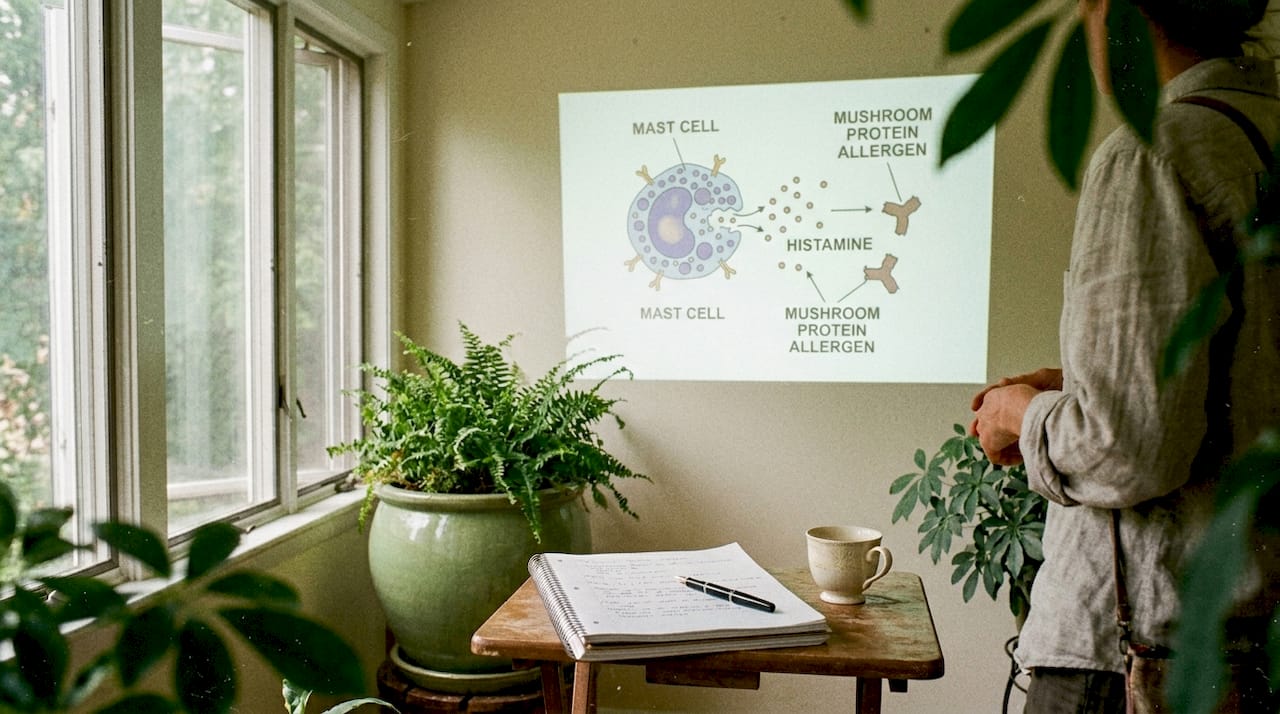
The reaction is classified as a Type I immediate hypersensitivity response. Symptoms typically appear within minutes to a few hours of ingestion or inhalation. The speed of onset is one of the clearest signals that a true IgE-mediated allergy is involved, as opposed to other types of mushroom reactions that develop over longer periods.
Mushroom proteins responsible for sensitization are found in both the fruiting body (the part you eat) and the spores. This means exposure can happen through eating, touching, or even breathing in spores near mushroom farms or during food preparation. Occupational exposure is a recognized risk factor, particularly for workers in mushroom cultivation facilities.
The body systems most commonly affected include:
- Skin: Hives (urticaria), eczema flares, contact dermatitis, and angioedema (swelling under the skin)
- Respiratory: Sneezing, nasal congestion, rhinitis, wheezing, and asthma-like symptoms
- Digestive: Nausea, vomiting, abdominal cramps, and diarrhea
- Systemic: Anaphylaxis, involving a sudden drop in blood pressure and airway constriction
Pro Tip: If symptoms appear within two hours of eating mushrooms and involve more than one body system at the same time, that pattern strongly suggests an IgE-mediated allergy rather than a sensitivity or intolerance. Document the timing and report it to an allergist.
How do mushroom allergies differ from shiitake dermatitis and sensitivities?
Not every adverse reaction to mushrooms is a true allergy. This distinction matters because the management strategies are completely different, and confusing them can lead to unnecessary dietary restrictions or, worse, a false sense of safety.
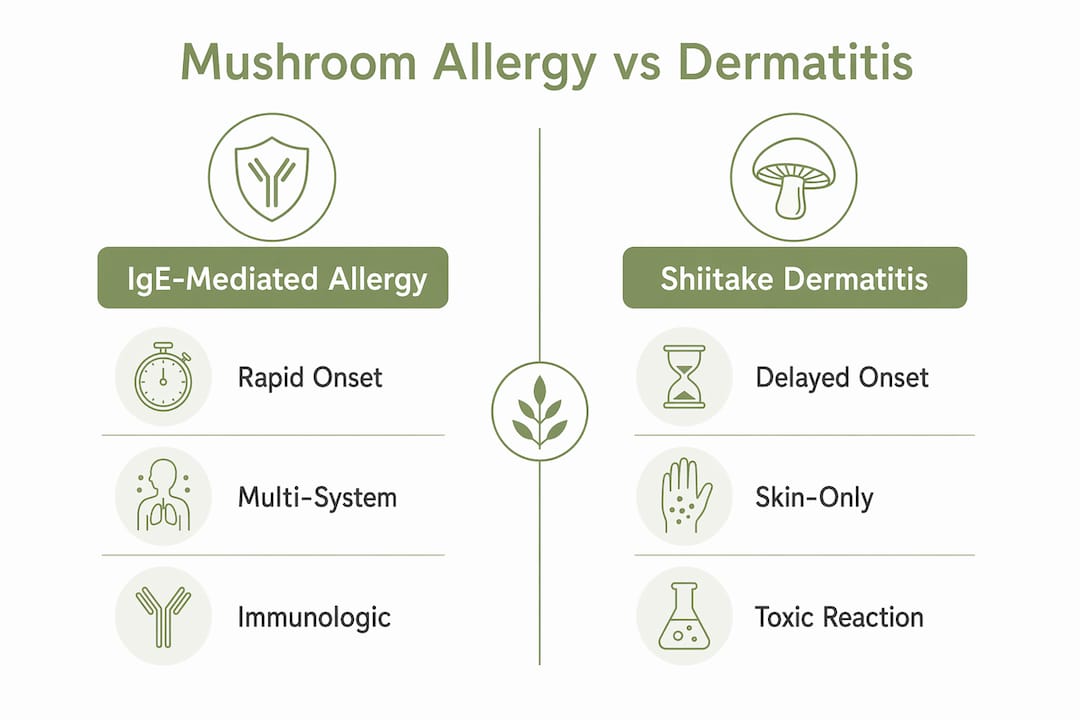
Shiitake dermatitis is a delayed toxic reaction, not an IgE-mediated allergy. It is caused by lentinan, a polysaccharide found in raw or undercooked shiitake mushrooms. The flagellate rash appears 24 to 48 hours after eating undercooked shiitake and presents as linear, scratch-like streaks across the torso, arms, and legs. It is self-limited, meaning it resolves on its own without treatment in most cases, and it carries no risk of anaphylaxis.
The table below summarizes the key differences between these reaction types:
| Feature | IgE-mediated allergy | Shiitake dermatitis | Mushroom sensitivity |
|---|---|---|---|
| Immune mechanism | IgE antibodies, mast cells | Toxic reaction to lentinan | Non-immune digestive response |
| Onset timing | Minutes to 2 hours | 24 to 48 hours | 30 minutes to several hours |
| Anaphylaxis risk | Yes | No | No |
| Skin presentation | Hives, angioedema | Linear flagellate rash | Rare |
| Prevented by cooking | No | Yes, thorough cooking deactivates lentinan | Partially |
Mushroom sensitivity and intolerance sit in a third category entirely. These are non-immune reactions, typically digestive, caused by difficulty breaking down certain mushroom compounds like chitin or sugar alcohols. They produce bloating, gas, and loose stools but no skin or respiratory symptoms and no anaphylaxis risk.
Pro Tip: Thorough cooking of shiitake mushrooms deactivates lentinan and prevents flagellate dermatitis. If you have experienced this rash only after eating raw or lightly cooked shiitake, fully cooking the mushroom may resolve the problem entirely without requiring avoidance.
What challenges exist in diagnosing mushroom allergenicity?
Diagnosing a true mushroom allergy is more complicated than a standard skin prick test or blood draw. The core challenge is that standard IgE testing using crude mushroom extracts frequently produces false positives. Crude extracts contain carbohydrate structures called cross-reactive carbohydrate determinants (CCDs). The body can produce anti-CCD IgE antibodies that show up as a positive result on a test even when no true clinical allergy exists. Recombinant protein testing improves specificity by isolating individual allergenic proteins, reducing the noise from CCD interference.
Component-resolved diagnostics (CRD) represent the current best practice in fungal allergy testing. Rather than testing against a whole mushroom extract, CRD tests against specific purified or recombinant proteins known to cause sensitization. This approach improves clinical relevance and helps clinicians distinguish between patients who are truly allergic and those who simply have cross-reactive antibodies with no clinical significance.
Cross-reactivity adds another layer of complexity. Fungi share allergenic proteins across species, meaning a person sensitized to one type of mold or mushroom may test positive for others without ever having been directly exposed. Shared allergenic proteins cause cross-sensitization, and not all mushrooms are equally allergenic to every individual. This is why broad dietary advice like “avoid all mushrooms” is often clinically inaccurate and unnecessarily restrictive.
Key diagnostic considerations include:
- Clinical history first: Symptom timing, severity, and the specific mushroom involved are the most important diagnostic data points
- Skin prick testing: Useful as a first screen but limited by extract quality and CCD interference
- Specific IgE blood testing: Standard serology with crude extracts has variable sensitivity and specificity
- Component-resolved diagnostics: The most precise available method for confirming true sensitization
- Oral food challenge: Conducted under medical supervision, this remains the gold standard for confirming or ruling out a clinical allergy
Combining detailed patient history with component-resolved testing gives clinicians the clearest picture of whether a true allergy is present and which mushrooms pose a genuine risk.
Which mushrooms are most commonly allergenic and what symptoms should you watch for?
Maitake and shiitake are the two most frequently reported allergenic mushrooms in clinical literature. Maitake allergy symptoms include hives, swelling, vomiting, and in severe cases, anaphylaxis, appearing within minutes to a couple of hours after ingestion. Shiitake can cause both IgE-mediated allergy and the separate toxic reaction described above, making it one of the more clinically complex mushrooms to assess.
Mushroom spores are a significant but underappreciated exposure route. Spore inhalation can trigger rhinitis, nasal congestion, and asthma-like symptoms in sensitized individuals, even without any ingestion. This is particularly relevant for people who cook with fresh mushrooms regularly or who work in environments where mushrooms are cultivated or processed.
Common mushroom allergy symptoms by category:
- Skin reactions: Hives, redness, itching, angioedema (swelling of lips, tongue, or throat), contact dermatitis
- Respiratory reactions: Runny nose, sneezing, nasal congestion, wheezing, shortness of breath, asthma flares
- Digestive reactions: Nausea, vomiting, stomach cramps, diarrhea
- Severe systemic reactions: Anaphylaxis, involving throat tightening, a sudden drop in blood pressure, rapid heartbeat, and loss of consciousness
The severity spectrum is wide. Some individuals experience only mild, localized hives. Others progress to anaphylaxis within minutes. There is no reliable way to predict severity based on prior mild reactions alone, which is why medical evaluation is critical for anyone who has experienced more than one reaction.
How can individuals with mushroom allergies safely manage their condition?
Safe management of a confirmed mushroom allergy requires a structured approach, not guesswork. The following steps reflect current clinical guidance:
- Get a confirmed diagnosis. Self-diagnosis based on symptoms alone is unreliable. Work with a board-certified allergist to confirm the allergy, identify the specific mushroom species involved, and assess cross-reactivity risk before making permanent dietary changes.
- Understand your specific triggers. Not all mushrooms carry the same risk for every individual. Personalized allergist evaluation integrating patient history, specific IgE testing, and clinical assessment is the most accurate path to identifying safe and unsafe species.
- Carry emergency medication if prescribed. Anyone with a confirmed IgE-mediated mushroom allergy and a history of moderate to severe reactions should carry an epinephrine auto-injector (such as an EpiPen) and know how to use it.
- Read labels carefully. Mushroom extracts and powders appear in supplements, broths, sauces, and seasoning blends. Check ingredient labels on packaged foods and dietary supplements before use. The mushroom supplement guide from Longevitybotanicals covers what to look for when evaluating mushroom-based products.
- Cook shiitake thoroughly if dermatitis is your only concern. If the reaction is shiitake dermatitis rather than a true IgE allergy, thorough cooking deactivates lentinan and typically prevents the rash entirely.
- Consult before using mushroom supplements. Functional mushroom supplements like Reishi, Lion’s Mane, Turkey Tail, Chaga, and Cordyceps are increasingly popular, but they contain the same proteins that can trigger reactions in sensitized individuals. Always consult an allergist before introducing any mushroom-based supplement.
Pro Tip: Before starting any mushroom supplement, use a mushroom wellness checklist to assess your personal risk factors and identify which species are most relevant to your health goals and allergy history.
Key takeaways
Mushroom allergenicity is an IgE-mediated immune response that requires accurate diagnosis, species-specific assessment, and a personalized management plan to avoid both unnecessary restriction and genuine health risk.
| Point | Details |
|---|---|
| IgE mechanism drives true allergy | Mast cell histamine release causes rapid symptoms affecting skin, lungs, and digestion. |
| Shiitake dermatitis is not an allergy | This delayed toxic rash from lentinan resolves with thorough cooking, not avoidance. |
| Crude extract tests have limits | Anti-CCD IgE causes false positives; component-resolved diagnostics improve accuracy. |
| Cross-reactivity complicates diagnosis | Shared fungal proteins mean one sensitization can produce positive tests for multiple species. |
| Personalized evaluation is required | Combining clinical history with specific IgE testing gives the most reliable diagnosis. |
Why the allergy-versus-reaction distinction matters more than most people realize
Most people who think they have a mushroom allergy have never had it confirmed by an allergist. That gap between perceived and confirmed allergy has real consequences. Unnecessary avoidance of all mushrooms means missing out on species with well-documented health benefits, including immune-modulating compounds like beta-glucans found in Turkey Tail and Reishi. At the same time, dismissing a genuine IgE-mediated reaction as “just a sensitivity” creates serious risk.
What the current research makes clear is that the diagnostic tools now available, particularly component-resolved diagnostics, are precise enough to give patients a real answer rather than a probability. The problem is that most primary care settings still rely on crude extract testing, which produces enough false positives to leave patients with an inaccurate picture of their actual risk.
The practical takeaway is this: if you have had a reaction to mushrooms, the most useful thing you can do is see a board-certified allergist, request component-resolved IgE testing where available, and bring a detailed record of your symptoms including timing, the specific mushroom, and how it was prepared. That information, combined with modern diagnostics, is what separates a well-managed allergy from a lifetime of unnecessary restriction or unmanaged risk.
— Recontour,
Mushroom supplements for sensitive individuals: options from Longevitybotanicals
For individuals who have confirmed their allergy status and want to explore functional mushroom products, Longevitybotanicals offers a range of high-quality options with transparent ingredient sourcing. The product catalog includes organic mushroom capsules, powders, and concentrated extracts covering species like Reishi, Lion’s Mane, Turkey Tail, Chaga, and Cordyceps. Each product category is clearly labeled by mushroom type, format, and intended benefit. Individuals with known sensitivities should consult a healthcare provider before use and review full ingredient lists carefully. Longevitybotanicals also provides educational resources to help consumers make informed decisions about mushroom-based supplementation.
FAQ
What is mushroom allergenicity?
Mushroom allergenicity is an IgE-mediated immune response to proteins in edible fungi, causing symptoms that affect the skin, respiratory system, and digestive tract within minutes to hours of exposure.
Are all mushrooms equally allergenic?
No. Species like shiitake and maitake are most commonly reported in clinical reactions, but cross-reactivity among fungi means sensitization to one species can produce positive test results for others without confirmed clinical allergy.
What is the difference between shiitake dermatitis and a mushroom allergy?
Shiitake dermatitis is a delayed toxic reaction to lentinan appearing 24 to 48 hours after eating undercooked shiitake. It is not IgE-mediated and carries no anaphylaxis risk, unlike a true mushroom allergy.
How is a mushroom allergy diagnosed accurately?
Accurate diagnosis combines detailed clinical history with specific IgE testing, ideally using component-resolved diagnostics rather than crude extracts, which are prone to false positives from anti-CCD IgE antibodies.
Can people with mushroom allergies use mushroom supplements?
Only after confirmed allergist evaluation. Mushroom supplements contain the same proteins that trigger IgE-mediated reactions, so individuals with a confirmed allergy should consult a healthcare provider before introducing any mushroom-based product.
Recommended
- Mushroom supplement dos and don’ts: safe guide for wellness – LongevityBotanicals
- Therapeutic mushrooms explained: benefits, science, and safe use – LongevityBotanicals
- How to safely incorporate daily mushroom intake for wellness – LongevityBotanicals
- Mushroom Dosage Explained: Finding Your Optimal Amount – LongevityBotanicals




